Lecture Details[]
Richard Loiacono; Week 4 MED1022; Pharmacology
Lecture Content[]
Nociceptive afferent neurons have a high threshold of stimulation. Prostaglandins are released in inflammation, can enhance effects of pain producing events. They facilitate the opening of voltage gated Na channels. NSAIDs can inhibit prostaglandins (anti-inflammatory, antipyretic, analgesic).
Opium has at least 20 different alkaloids. They are a combination of euphoric and depressive agents. They are agonists at receptor systems. Mu opioids have most of the major effects of opioids (analgesia, cough suppression) and some adverse effects (resp depression, sedation, dependence and euphoria). Delta and kappa receptors contribute to analgesic effect.
{kind=link}
Opioid receptors are coupled to Gi, decreased cAMP levels; activates K channels to hyperpolarise and reduces Ca current by inhibiting Ca channels. Morphine mimics endogenous opioids (endorphins, enkephalin) which are small peptides. It modulates pain and is involved in exercise addiction.
Fast pain throgh Adelta is not modulated by opioids, slow pain (C fibres) is. Gate theory is that SG is rich with endogenous opioids; they inhibit transmission to afferent neurons at 'the gate'. Exogenous opioids target opioid receptors.
Opioids can also act at PAG; enriched in opioid receptors- recieves nociceptive signal from periphery, modulatory input from the cortex.
Analgesia helps pain of terminal illness and cancer pain, postoperative pain, headache, obstetrical analgesia. They also cause euphoria/dysphoria, resp depression, depression of cough reflex, sedation. Inhibits GIT motility and increases tone. Constricts pupils. Nausea and vomiting can occur due to CTZ stimulation and release of histamine (may be specific to morphine/heroin). This can lead to urticaria and itching, bronchoconstriction and hypotension. Acute OD (resp depression) is treated with opioid receptor antagonist (naloxone).
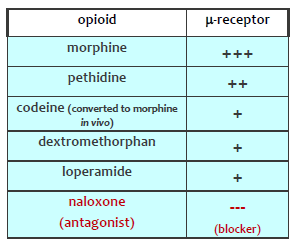
Pethidine has a much shorter duration than morphine (2-3 not 3-6). Codeine is rarely addictive and 10-20% as potent as morphine. Dextromethorphan is cough suppressor (elevates threshold). Loperamide is poorly absorbed so effects are confined to GIT. Tramadol enhances central serotonin transmission, weak mu opioid receptor agonist and is used for chronic pain (less resp depression, less dependance). Naloxone inhibits endogenous opioids, can be used in withdrawal and dependance treatment.
Heroin is lipid soluble, hydrolysed to morphine in the brain. Lasts 3-5 hours. Cross tolerance can occur between opioids. Methadone is a drug used for cross tolerance to prevent severe withdrawal, lasts 36 hours.
Conotoxins block N-type Ca channels which control neurotransmitter release at spinal synapses.