Lecture Details[]
Norm Eizenberg; Week 4 MED1011; Anatomy
Lecture Content[]
Muscle can be skeletal, cardiac or smooth. Skeletal muscle has tendinous attachments to bone and a large tendon to a developing bone is likely to be associated with a traction epiphysis. It contains epimysium, perimysium and endomysium. They can have both fleshy insertions at the bellies or tendinous insertions at the tendon.
Muscle bellies can be fusiform, digastric, tendinous insertions or circular; shapes can be strap, triangular, rhomboid or quadrate. Regressive variations are evolutions for a longer or shorter tendon, atavistic variation splits tendons to form ligaments and shorter tendons. Degrees of muscle injury can be a sprain (I), partial tear (II, pain in strength testing and when stretched) or complete tear (III, total loss of function). A muscle can tear in its belly, musculotendinous junction or tendon. A tear is likely to occur at a site of a previous scar. An avulsion fracture is when a fragment of bone is torn away.
Fibrous muscle specialisations can be raphes thin tissue of attachment), aponeuroses (flat sheets of attachment) or multiple tendons. Tendons tend to occur at sites of pressure or friction. Deep fascia is a continuous sheath found around parts of the body that expand significantly. It is not found over the subcutaneous surface of a bone. Retinaculum is flexor deep fascia, retinacula is extensor. Fascial septum separates compartments. Where nerves and vessels have a common course they tend to share a fascial shealth. Muscles that share an action are generally divided by sheaths into the same compartment.
Fibrous tendon sheaths enclose long flexor tendons, forms roof of the fibro-osseous tunnel where tendons lie. It is thicker over the phalanx and thin/lax over joints. It contains a synovial tendon sheath which is a tubular serous membrane that surrounds a tendon and minimises friction. It occurs at sites where tendons pass under ligaments or retinacula and where tendons pass through osseofibrous canals. A synovial sheath develops by slowly invaginating a tendon. A mesotendon is blood supply to a tendon, a synovial sheath grows around it. Interruption of this blood supply may lead to tendon rupture.
Irritation by unaccustomed or repetitive movement may lead to tenosynovitis with accumulation of fluid or pus. Inflammation of the tendon sheath may also be associated with inflammation of tendon (tendinitis) or of its fibrous tendon sheath (tenovaginitis). Infection may spread alon a synoial sheath.
{kind=link}
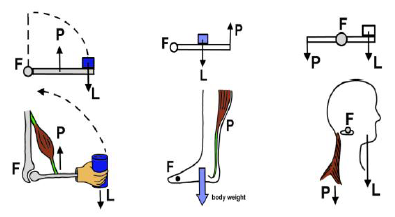
3rd order levers are for range and speed, eg a bicep. 2nd order are for power, eg standing on toes. 1st order are for balance, eg tilting head. Leverage is determined by distance of line of pull from the axis of movement (joint). Stretching creates stronger contraction due to overlap of myofilaments. Muscles crossing more than one joint enable extra force to be generated. They are particularly prone to injury from over stretching (by collective movement at the two joints).
Muscle fibres parallel to the line of pull allow a greater range of movement, those oblique increase strength but decrease range of movement. They can be divided into unipennate, bipennate and multipennate partitions. The active range of movement is proportional to the length of the mucle belly, and the strength is proportional to the cross-sectional area.
{kind=link}
Concentric contraction is where muscle as a whole shortens to move a load (picking something up). Isometric contraction is where the muscle maintains the same length while the muscle fibres contract without movement. Eccentric contraction is where muscle lengthens while muscle fibres contract with movement against gravity eg. while lowering a load. Prime mover is the muscular contraction directed to production of a particular movement. Antagonist lengthens in a contraction of prime mover (reverse in eccentric contraction). Isometric is where both agonist and antagonist contract to stabilise the joint. Restriction of prime mover occurs when antagonist is unable to stretch or relax sufficiently.
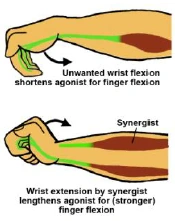
A fixator is a short muscle located close to the axis of movement, blends with the joint capsule and stabilises joint by acting as a dynamic ligament. Synergist action prevents excessive shortening of prime mover when it acts at two joints and is trying to use distal joint, does so by opposing unwanted movement at the proximal joint (is an antagonist there).
Passive insufficiency is due to antagonist being able to relax or contract sufficiently, active insufficiency is when prime mover is too shortened, causes weakening of contraction (can also be from no myofilament overlap). The hilum is where the nerve, artery and vein enter. It is generally near the middle of the muscle belly on its deep surface. A motor unit is a group of muscles innervated by one nerve and is tested near the hilum.

{kind=link}
Muscle tone is resistance to stretch, in under reflex control and is modulated by the recruitment of motor units. Muscles with a common action share a nerve supply. Nerve supply reflects developmental origin. A muscle located on the border of two compartments may have dual supply. Myotomes are muscles supplied by particular spinal cord segments. Proximal muscle groups are more cranial than distal muscle groups.
Vascular supply is rich to muscle belly, poor to tendon. In muscle injuries healing of muscle injury (with considerable bleeding due to vascular supply) tends to leave fibrous scar tissue as completely torn muscle fibres do not regenerate. Scar tissue is weaker than muscle and shortens it, predisposing to future injury.